FAQ
Why isn't taking calcium enough for bone health?
Calcium is crucial for bone metabolism and bone health, but alone it is not enough. In fact, well-publicised studies have shown that rather than going directly to bones, calcium gets sidetracked, building up in arteries and soft tissues, a leading cause of heart attack or stroke in older adults. This is referred to as the “Calcium Paradox.”
Vitamin K2 is the missing piece of the equation:
- -Bone Health: The entire skeleton is replaced every seven years – the process is regulated by osteoblasts (cells that build up the skeleton) and osteoclasts (cells that break down the skeleton). Osteoblasts produce osteocalcin, a K vitamin-dependent protein that helps bind calcium to the bone matrix, increasing bone mineral content and making the skeleton less susceptible to fracture.
- -Cardiovascular Health: Vitamin K2 also activates the matrix Gla protein (MGP), which research has shown to be the most potent inhibitor of vascular calcification. So with osteocalcin and MGP activated, calcium is directed away from the arteries (where it doesn’t belong) and to the bones (where it does belong).
Is the difference between K1 and K2 simply the time in the body? Do both forms have the same action?
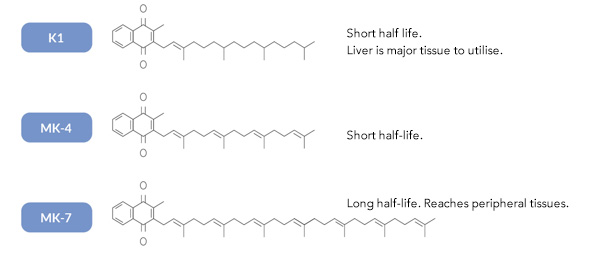
Phylloquinone (vitamin K1) has a short half-life and mainly concentrates in the liver where it is essential for blood clotting. Menaquinones (vitamin K2 family) have a longer side chain than vitamin K1, which means they have a much longer half-life and therefore can get to bones and soft tissues where they can be used for calcium utilisation.
At this stage it appears that both K1 and K2 do have some similar properties however due to the longer half-life of the menaquinones they are more active in calcium utilisation. There is evidence emerging to suggest that K2 has properties that K1 is not necessarily involved with (particularly in relation to things like down-regulation of NFkB and TNF-alpha, activation of Matrix Gla protein and brain cell mitochondria function etc).
Is K2 better than K1?
The question is not about vitamin K2 being better than vitamin K1 its rather about the function and what each is more useful for. Vitamin K1 has a short half-life and mainly concentrates in the liver where it is essential for blood clotting. Vitamin K2 has a much longer half-life than vitamin K1 and therefore gets to bones and soft tissues where it can be used for calcium utilisation.
Do K1 and K2 work together?
A number of population-based studies have investigated the beneficial health effects of high vitamin K intake. Some studies have only focused on vitamin K1, but in all studies in which K1 and K2 were measured separately, the health effects of K2 were more prominent than those of K1. Moreover, the limited data available suggest that the “long-chain” menaquinones (MK-7, MK-8, and MK-9) are the most active compounds for health effects beyond haemostasis.
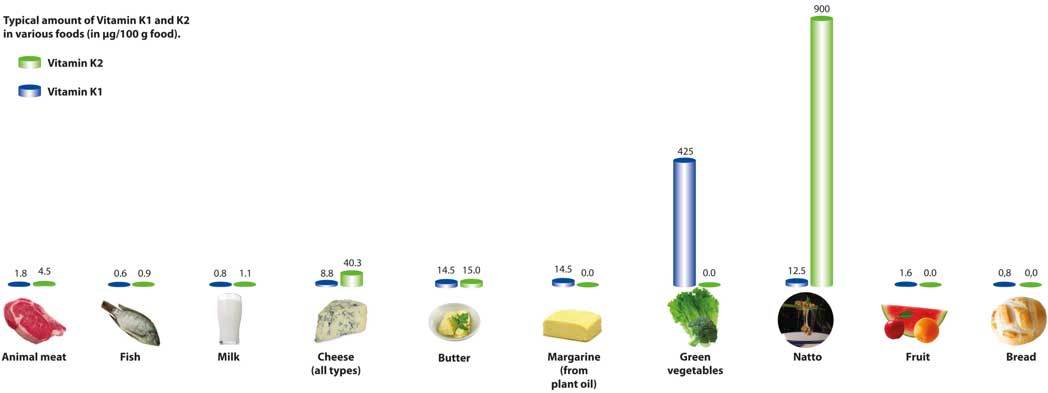
Can I find vitamin K2 in food or only in bottles?
Attaining adequate vitamin K2 from diet is ideal. Unfortunately, that just isn’t terribly likely. For example, one of the best sources of vitamin K2 in Western society is from fermented cheeses. In order to attain an effective amount of vitamin K2 (studies have shown as little as 45 -50 mcg of vitamin K2 can produce the desired effect), one would have to consume 59g of hard cheese a day.
So, obtaining optimal amounts of vitamin K2 through diet alone is difficult, which makes supplementation a viable alternative. The most desirable form of vitamin K2 is natural vitamin K2 as MK-7, as this is the most bioavailable, bioactive, and longest-lasting form.
NattoPharma, an international biotechnology company and exclusive supplier of MenaQ7®, the original vitamin K2, has long partnered with Maastricht University in The Netherlands, which is the world’s largest research institute dedicated to vitamin K2. These scientists have produced findings that clearly demonstrate not only vitamin K2’s role in bone health, but that it is safe and effective for children.
Are there any known contraindications for vitamin K2?
The only contraindication for vitamin K2 is the use of coumarin derivatives as oral anticoagulants. These are vitamin K2 antagonists and therefore cannot be used with vitamin K2. This group of drugs includes warfarin.
Fortunately, today we are seeing a new generation of oral anticoagulants that are direct thrombin and factor Xa inhibitors. These drugs can be combined with vitamin K without hesitation.
Heparin produces its major anticoagulant effect by inactivating thrombin and activated factor X (factor Xa) through an antithrombin (AT)-dependent mechanism. So, in our opinion, it is safe to use with K.
It is always best for to consult your prescribing GP before adding a K2 supplement, particularly if you are on oral anticoagulants.
Should vitamin K2 only be offered where low bone density has been diagnosed?
Vitamin K2 requirements are higher in children and menopausal women. Dietary intake and family history of low bone density should be taken into account. Epidemiological studies suggest that most people on a standard western diet are deficient to some extent in vitamin K2. As with osteoporosis and cardiovascular disease it is better to strike before symptoms are presenting because that usually means the conditions are drastically advanced.
What is the timeframe for bone mineral density improvement?
The resorption process (i.e., break down) of bones is a natural process, but it is very slow. If you are an adult, your bone becomes less dense each year. While this happens very slowly, over many years it can lead to osteoporosis and fractures.
Vitamin K2 has been shown to effectively decrease the bone resorption process. The process was significant after 3 years of treatment with nutritional dosage (180 mcg) of vitamin K2 – MK-7.
It is likely that one can expect a faster effect if they take a higher dose, and if they are physically active and consuming a “healthy diet.”
What effects does K2 have on osteoporosis and how soon should patients see an improvement?
From a scientific perspective there is no evidence to suggest that you can completely reverse osteoporosis. However, studies have shown that vitamin K2 can slow the process of bone resorption and decrease the risk of fracture.
Research suggests that at a dose of 180mcg daily maximal levels of osteocalcin carboxylation are reached after 1 year of supplementation and are maintained by supplementation after that. Effects of MK-7 supplementation on bone mass are seen only after 2 years of supplementation. The Knapen et al. (2013) study showed that only after 3 years of supplementation did the bone health start to improve compared to placebo. In the Knapen study there were significant difference at the site of the lumbar spine after the first year of supplementation for bone mineral content BMC and after the second year for bone mineral density (BMD).
What is the timeframe for cardiovascular benefits?
In healthy volunteers, a biochemical effect (i.e., improved activation of the vascular calcification inhibitor Matrix Gla Protein, or MGP) is seen within 6 weeks, with a maximal effect after 3 months. It is suggested that from that time on there will also be a clinical benefit for the subject, but these processes proceed slowly and a measurable benefit in a clinical trial (vitamin K2 over placebo) becomes visible after at least one year, with a more pronounced effect after 2 and 3 years.
Is it necessary to stay with the 180mcg dose or will increased dose improve results?
Research has shown that there is no perceived added benefit of dosing any higher than 180mcg. Blood and tissue levels reach acceptable levels within 3 months and increasing dose does not improve that.
Is it safe for children?
Yes! Children have much higher bone metabolism than adults, which means they need more vitamin K to build healthy bone tissue. The higher peak bone mass they achieve, the lower the risk of poor bone health and potentially osteoporosis later in life. Unfortunately, food consumption statistics indicate that vitamin K intake is declining in Western societies. A dose of 45mcg daily would be a satisfactory dose for children however the TGA do not allow labeling for children at this stage.
Who does it benefit?
Before the advent of processed foods, diets provided adequate amounts of vitamin K2, but fast-paced lifestyles have us dependent on convenient, nutrient-lacking foods that have led to dire deficiencies, particularly in children, which leads to unhealthy adults. In fact, recent studies show that adults above the age of 40 are second only to children when it comes to having the largest vitamin K2 deficiency. Studies show that improving vitamin K status in children over a 2-year period resulted in stronger, denser bones.
Natural versus synthetic?
Bioavailability studies show that all-trans synthetic vitamin K2 as MK-7 has a similar bioavailability profile to natural vitamin K2 as MK-7.